Pulse Oximetry Protocols
Protocols
The following are protocols developed by Newborn Screening Ontario (NSO) for pulse oximetry screening.
- CCHD Protocol - an overall screening protocol
- SCN/NICU Protocol - a specific guideline for screening special care babies
- Early Discharge Protocol - a specific guideline for screening babies who are discharged from hospital before 24 hours
- Community Screening Protocol - a specific guideline for screening babies in a non-hospital environment
- Screen Positive Protocol - a guideline for evaluation and management for health care providers who obtain a CCHD screen positive
- Recommendations for CCHD Screening in the Presence of a Murmur - a guideline for performing CCHD screening in the presence of a heart murmur
Pulse oximetry screening
A pulse oximeter is a medical instrument that measures the amount of oxygen that is carried by hemoglobin. A pulse oximeter measures the colour of the blood flowing through the capillaries of the skin and analyzes it, expressing it as a percentage of saturation (for example , fully saturated hemoglobin would be SpO2 100% or Saturation, pulse, of Oxygen 100%).
Because the blood is pulsating, a heart rate can also be obtained through pulse oximetry.
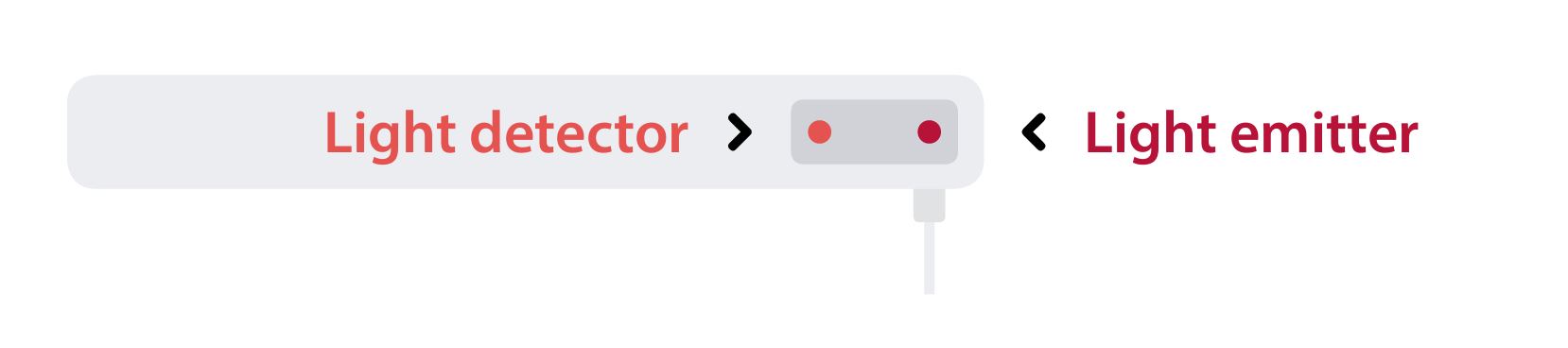
A pulse oximeter has a probe with both a light emitter and a light detector. The probe is applied to the skin so the light can shine through, and be reflected off the red blood cells in the capillaries. The light is received by the detector and the monitor can convert the reading into a number or percentage saturation.
Probe placement: pre-ductal vs post-ductal
Probe placement is important. Thinner tissue with capillary beds close to the skin’s surface makes it easier for the probe to read the blood colour. The emitter and the detector must be directly opposite each other for an effective reading.
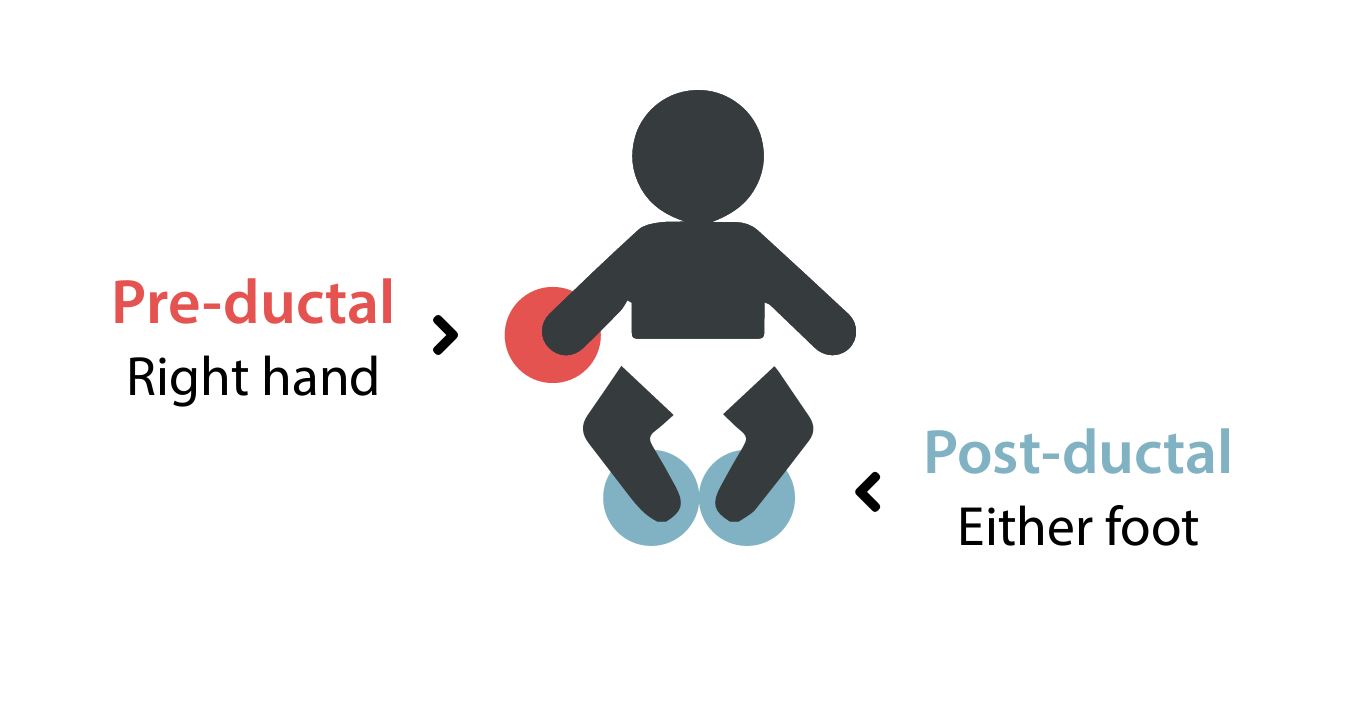
For CCHD screening the required site placement is the right hand and either foot.
- The right hand is PRE-DUCTAL. This means that the blood that flows to the right hand leaves the aorta before the ductus arteriosus.
- Either foot is a POST-DUCTAL site, as the blood flow to the lower extremities leaves the aorta after the ductus arteriosus. This blood may be mixed with blood from the pulmonary vessels through the ductus arteriosus if the ductus has not closed, resulting in lower oxygen levels.
Screening after 24 hours is recommended as the ductus is most likely closed at this point. Thus a difference in oxygen levels pre-ductally and post-ductally warrants further investigation.
Signal reliability
There are a few ways to ensure the monitor is relaying an accurate reading (some are specific to the brand and model of monitor and will have manufacturer-specific instructions).
To obtain an accurate reading, ensure that:
- The initial and regular maintenance and quality assurance of the monitor is complete and up to date;
- The infant is calm and not moving excessively, the probe placement is secure (light emitter and receptor are aligned);
- There is an even, regular pleth line waveform (movement and unstable signals will give an irregular, ‘dancing’ line);
- There is an audible, regular heart rate (unstable signals or movements may elicit an irregular audible beat);
- The number reading is steady (not jumping around and somewhat random in nature) and consistent with other heart rate monitors.
Factors that affect SpO2
To obtain an accurate pulse oximetry measurement, the infant should be in a warm, calm, non-fussing state.
These factors can affect SpO2 measurement:
- Perfusion: Well-perfused tissue will be read more effectively by the monitor. The capillary bed refill time is ideally 2- 3 seconds; however, the monitors recommended for CCHD screening should still function in low-perfused tissue.
- Temperature: The infant’s temperature should be within normal range (36.5°-37.5° C). A cooler temperature can affect the perfusion to the extremities, thus affecting the saturation reading.
- Phototherapy lights: The pulse oximetry probe emits a light that passes through the tissue and is picked up by a detector piece. Phototherapy light can interfere with the probe detector and disrupt the reading of the oxygen saturation. Please turn off phototherapy lights prior to conducting the CCHD screen. Resume the treatment once the screen is complete.
- Movement of the limb: The pulse oximeter reads by picking up the flow of blood through an arterial pulse; the reading is most reliable when the limb is still. Try bundling the infant once the probe is applied to ensure a reliable reading.
- Probe placement: The probe should be applied to the thin part (non-thumb side) of the right hand or the thin part (outer aspect) of the foot. The light emitter and the light detector should be facing each other to ensure the signal can be received.
Contact NSO
Subscribe to the Submitter Bulletins to stay up to date on the latest newborn screening updates, or submit a question about newborn screening.